Background
Background
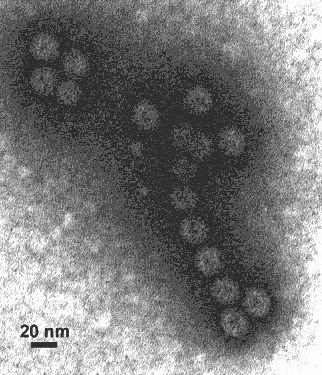
The unprecedented 2014 epidemic of Ebola virus disease (EVD) has prompted an international response to accelerate the availability of a preventive vaccine. A replication-defective recombinant chimpanzee adenovirus type 3-vectored ebolavirus vaccine (cAd3-EBO), encoding the glycoprotein from Zaire and Sudan species that offers protection in the nonhuman primate model, was rapidly advanced into phase 1 clinical evaluation.
Methods
We conducted a phase 1, dose-escalation, open-label trial of cAd3-EBO. Twenty healthy adults, in sequentially enrolled groups of 10 each, received vaccination intramuscularly in doses of 2×1010 particle units or 2×1011 particle units. Primary and secondary end points related to safety and immunogenicity were assessed throughout the first 4 weeks after vaccination.
Results
In this small study, no safety concerns were identified; however, transient fever developed within 1 day after vaccination in two participants who had received the 2×1011 particle-unit dose. Glycoprotein-specific antibodies were induced in all 20 participants; the titers were of greater magnitude in the group that received the 2×1011 particle-unit dose than in the group that received the 2×1010 particle-unit dose (geometric mean titer against the Zaire antigen, 2037 vs. 331; P=0.001). Glycoprotein-specific T-cell responses were more frequent among those who received the 2x1011 particle-unit dose than among those who received the 2×1010 particle-unit dose, with a CD4 response in 10 of 10 participants versus 3 of 10 participants (P=0.004) and a CD8 response in 7 of 10 participants versus 2 of 10 participants (P=0.07).
Conclusions
Reactogenicity and immune responses to cAd3-EBO vaccine were dose-dependent. At the 2×1011 particle-unit dose, glycoprotein Zaire-specific antibody responses were in the range reported to be associated with vaccine-induced protective immunity in challenge studies involving nonhuman primates. Clinical trials assessing cAd3-EBO are ongoing. (Funded by the Intramural Research Program of the National Institutes of Health; VRC 207 ClinicalTrials.gov number, NCT02231866 .).
REFERENCE: