Este artículo es sobre soluciones desinfectantes, siga el link para ver:
Publicado originalmente el 19 de Julio de 2008.
Actualizado 03/feb/2025
El hipoclorito de sodio (NaOCl) es un compuesto oxidante de rápida acción utilizado a gran escala para la desinfección de superficies, desinfección de ropa hospitalaria y desechos, descontaminar salpicaduras de sangre, desinfección de equipos y mesas de trabajo resistentes a la oxidación, eliminación de olores y desinfección del agua. Los equipos o muebles metálicos tratados con cloro, tienden a oxidarse rápidamente en presencia de hipoclorito de sodio.
El hipoclorito de sodio es vendido en una solución clara de ligero color verde-amarillento y un olor característico. Como agente blanqueante de uso domestico normalmente contiene 5-6.5% de hipoclorito de sodio (con un pH de alrededor de 11, es irritante y corrosivo a los metales). Cuando el hipoclorito se conserva en su contenedor a temperatura ambiente y sin abrirlo, puede conservarse durante 1 mes, pero cuando se ha utilizado para preparar soluciones, se recomienda su cambio diario. Entre sus muchas propiedades incluyen su amplia y rápida actividad antimicrobiana, relativa estabilidad, fácil uso y bajo costo.
El hipoclorito es letal para varios microorganismos, virus y bacterias vegetativas, pero es menos efectivo contra esporas bacterianas, hongos y protozoarios. La actividad del hipoclorito se ve reducida en presencia de iones metálicos, biocapas, materiales orgánicos, bajo pH o luz UV. Las soluciones de trabajo deben ser preparadas diariamente. El cloro comercial que contiene 5-6%, que será utilizado para la desinfección de superficies, debe ser diluído 1:10 para obtener una concentración final de aproximadamente 0.5% de hipoclorito. Cuando se quiere desinfectar líquidos que pueden contener material orgánico, debe tenerse una concentración final de 1% de hipoclorito.
Gracias a su alta disponibilidad continua siendo de alto uso en hospitales. Pueden encontrar otras características y hojas de seguridad del hipoclorito de sodio.
El modo de acción del hipoclorito es la oxidación: oxida proteínas, oxida DNA y RNA, oxida grasas, oxida metales.. OXIDA!, OXIDA!, OXIDA!, OXIDA!, OXIDA!...
.png)
RECOMENDACIONES PARA LA PREPARACIÓN Y USO:
.png)
#VIDEOBLOG:
------------------------------------------------------------------------
CONCENTRACIONES RECOMENDADAS
- Venta al público: (Blanqueador casero, presentación comercial): 5-6 % (50-60 g/l, 50,000 ppm) de cloro libre
- Para desinfección con material orgánico o derrames: 1% (10 g/l, 10,000 ppm)
- Para desinfección general de áreas sin materia orgánica: 0.5% (5g/L; 5,000 ppm)
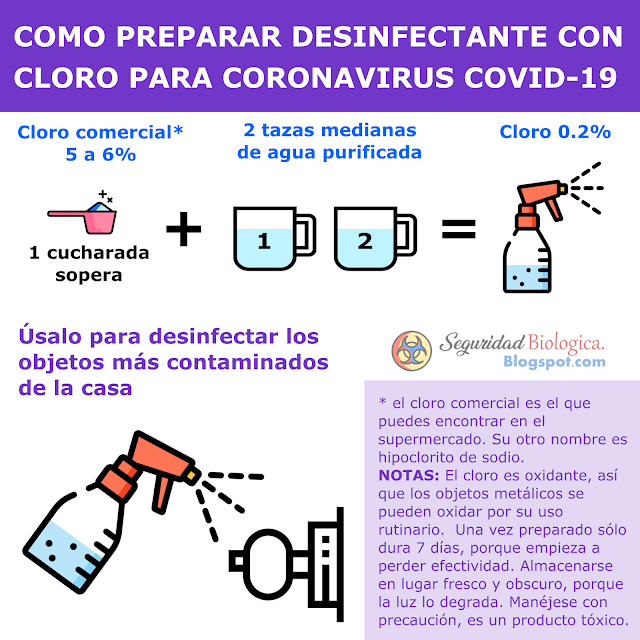
- Para desinfección de superficies (CORONAVIRUS): 0.2%
- Para limpieza general, desinfección de manos, desinfección de ropa: 0.05% (500 mg/L; 500 ppm) *
-----------------------------------------------------------------------
RECOMENDACIONES PARA LA PREPARACIÓN Y USO:
- Antes de elegir un agente desinfectante, por favor revisa su efectividad para el microorganismo que te interesa.
- USAR agua destilada o desinizada. El agua de la llave contiene muchos metales y sales que interfieren con su efectividad.
- Revisar la etiqueta antes de preparar el hipoclorito de sodio buscando la caducidad y la concentración de venta.
- Existen dos tipos de hipoclorito de sodio. El regular, que tiene una caducidad de 2 a 3 meses, y el "estabilizado", que tiene una caducidad de 1 a 2 años. Pero ambos se degradan rápidamente una vez preparados, por lo que no deben utilizarse después de 5 días de su preparación.
- Almacenar en un lugar fresco, seco y obscuro, ya que la luz y el calor aceleran su degradación.
- Existen varios procedimientos para la desinfección, por ejemplo LAVADO => DESINFECCIÓN => ENJUAGUE, es decir, realizar un lavado antes de la desinfección para retirar materia orgánica, luego aplicar el desinfectante, y realizar enjuagado para eliminar el exceso de desinfectate.
- Para la desinfección de líquidos que puedan contener microorganismos, debe prepararse una solución al 2% de hipoclorito de sodio. Posteriormente, mezclar en proporción 1:1 (1 volumen de desinfectante, 1 volumen de líquido). De esta forma, al final tendrá una concentración de 1%. Dejar reposar durante 30 minutos. Por ejemplo: 200 ml de orina + 200 ml de solución de hipoclorito de sodio al 2%.
- Para desinfectar superficies o materiales de laboratorio (que no sean metálicos), que no contengan material orgánico, deberá usarse una solución de hipoclorito de sodio al 0.5%. Por ejemplo, para desinfectar gradillas de laboratorio de plástico, sumérjalas en la solución al 0.5% por al menos 30 minutos.
-----------------------------------------------------------------------
FÓRMULA PARA PREPARAR SOLUCIONES DESINFECTANTES

Cualquier concentración puede ser utilizada para obtener una solución de hipoclorito diluída utilizando la siguiente fórmula: =>
Por ejemplo para preparar una solución 0.5% a partir de una 4.5% de hipoclorito de sodio se utilizarán 8 partes de agua con 1 parte de hipoclorito de sodio.
Donde "parte" puede ser utilizado para cualquier unidad de medida (litro, mililitro, galones, etc), o utilizando cualquier medidor (taza, frasco, garrafón, etc). En países de habla francesa, la cantidad de hipoclorito se expresa como "grados de cloro". Un grado de cloro = 0.3% de cloro activo. (Ref. 8)
Otra fórmula para calcular el volumen necesario para preparar el hipoclorito de sodio 0.5% a partir de una solución concentrada:




PREPARACIÓN RÁPIDA DE HIPOCLORITO DE SODIO

DESINFECCIÓN DE SÁBANAS Y ROPA DE CAMA Otra fórmula para calcular el volumen necesario para preparar el hipoclorito de sodio 0.5% a partir de una solución concentrada:

REVISAR LA ETIQUETA PARA VER LA CONCENTRACIÓN DE CLORO



DESCARGAR AQUI TABLA PARA PREPARAR HIPOCLORITO DE SODIO CON FINES DE DESINFECCIÓN PDF
------------------------------------------------------------------------
------------------------------------------------------------------------
PREPARACIÓN RÁPIDA DE HIPOCLORITO DE SODIO

En el caso de coronavirus COVID-19 las concentraciones consideradas efectivas es a partir del 0.2%. El tiempo de contacto recomendado es de 2 a 5 minutos.

--------------------------------------------------------------------
--------------------------------------------------------------------
Toda la ropa de cama que ha estado en contacto con pacientes puede estar contaminado con líquidos o fluidos corporales (orina, sangre, vómito). Cuando se manejan este tipo de ropa, debe utilizarse equipo de protección adecuado, pero debe incluirse, guantes, mascarillas, lentes de protección, batas y botas. Los excesos de excremento deberán retirarse y colocarse en bolsas para desechos. Antes de desinfectar, deberá realizarse un lavado en lavadora con agua y jabón. Enjuagar para eliminar el exceso de jabón. Finalmente, colocar las sábanas en una solución de hipoclorito de sodio al 0.05%, durante por lo menos 30 minutos ó una hora. Puede realizarse un segundo enjuague para eliminar el exceso de hipoclorito, y continuar con los procesos normales de secado.
El lavado a mano debe evitarse en la medida de lo posible. Cuando por las condiciones, no puede utilizarse lavadoras automáticas, las sábanas deberán colocarse en un gran contenedor con agua caliente y jabón, y agitar en círculos con un palo o varilla. Eliminar el agua, y colocar una solución al 0.1% de hipoclorito de sodio por 15 minutos, sumergiendo completamente las sábanas. Enjuagar nuevamente y dejar secar, evitando sacudir en la medida de lo posible (Ver Ref. 8).
------------------------------------------------------------------------
SOBRE LA INESTABILIDAD DEL CLORO:
Una vez preparadas, las soluciones comunes de hipoclorito de sodio guardadas a 25ºC, en recipientes cerrados, contenedores opacos, pierden 50% de su contenido de cloro libre en un periodo de 30 días. Una solución al 1%, tendrá solo 0.5% de cloro 30 días después de preparado. Las soluciones al 5% se degradan más lentamente si se almacenan en contenedores obscuros. A mayor temperatura y con mayor cantidad de luz que reciban, el proceso de degradación se acelera (Ref. 6).
Existen soluciones "estabilizadas" de hipoclorito de sodio, que tienen una caducidad mínima de 1 año. Estas soluciones deben mantenerse a menos de 25ºC, lejos de la luz del sol y son comercializadas con ese nombre de "estabilizadas". Estas soluciones se mantienen estables mientras se encuentran bien cerradas en su envase original, ya que una vez que se preparan soluciones a partir de ellas, comienza su proceso de rápida degradación, debido a que los "estabilizadores" se diluyen. El hipoclorito de sodio normal se degrada rápidamente (Ref. 11).
---------------------------------------------------------------------
SOBRE LA TOXICIDAD DEL CLORO:
El hipoclorito de sodio ocasiona:
- Irritación ocular, orofaríngea, esofagial y quemaduras gástricas.
- Corrosión a los metales
- Reacciona de forma tóxica con el amoniaco y ácidos (presente en los productos desinfectantes comunes), por lo que no deben hacerse mezclas de desinfectantes.
- Producción de carcinógeno bis (clorometil) eter cuando se mezcla con formaldehído.
- Producción de carcinógeno trihalometano cuando el agua es hiperclorinada (exceso de cloro).
- Para la potabilización del agua, la NOM-127-SSA1-2021, establece que debe vigilarse los residos producto de la clorinación tales como: [1] Cloro residual libre, tabla 9; [2] trihalometanos (Bromodiclorometano, Bromoformo, Cloroformo y Dibromoclorometano), tabla 10, [3] ácidos haloacéticos (Ácido cloroacético, Ácido dicloroacético, Ácido tricloroacético), tabla 11.
Por favor visite esta página para ver las características y tratamiento de la intoxicación por cloro: https://medlineplus.gov/spanish/ency/article/002772.htm

Revista del consumidor Mayo 2020.
WEBINAR: Toxicidad del Dióxido de Cloro
-----------------------------------------------------------------------
REFERENCIAS: